
Femoral Neck Fracture Causes, Symptoms & Treatment Options
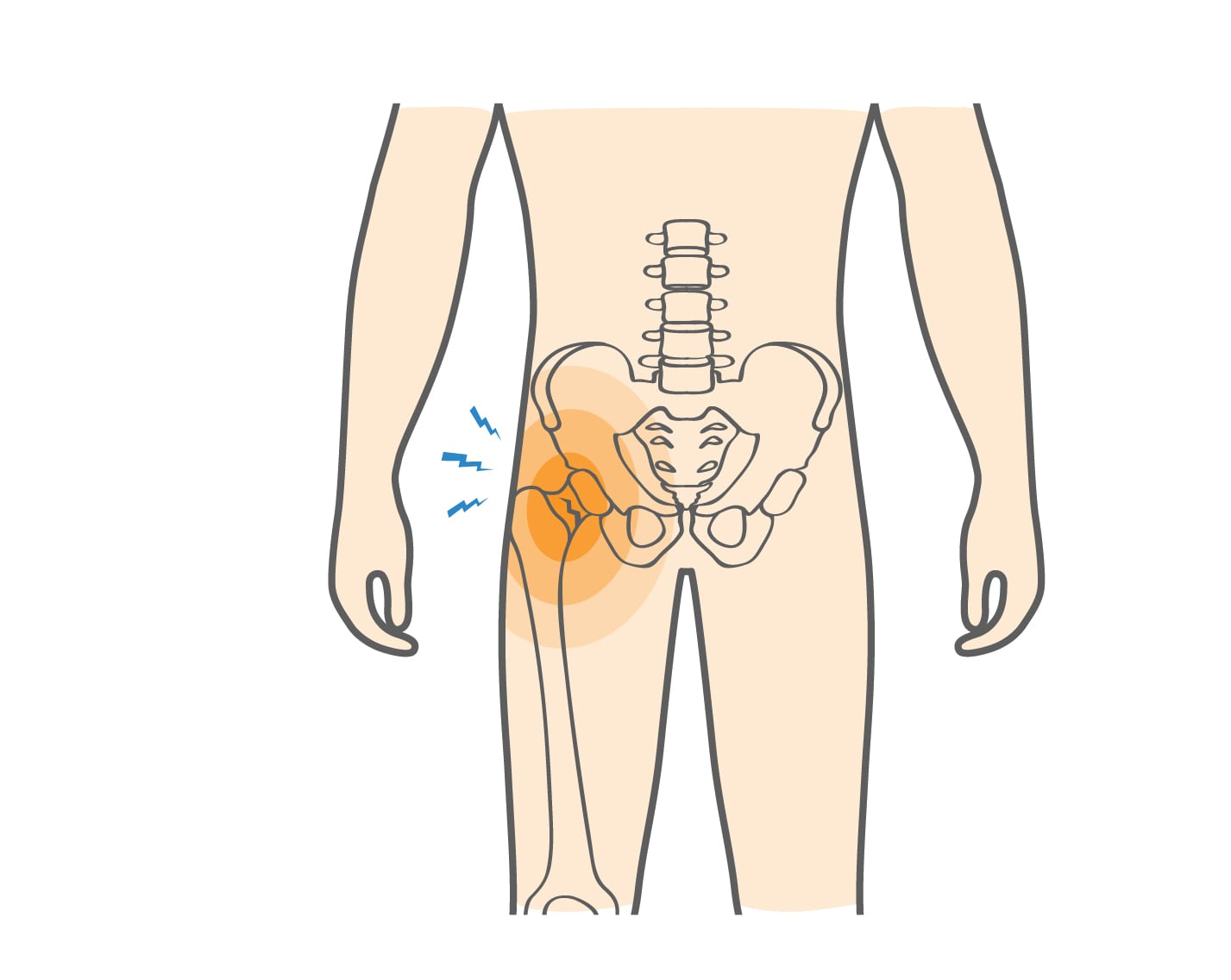
A femoral neck fracture is a break in the short, narrow section of the femur that connects the rounded femoral head to the long femoral shaft. The femur is the strongest and largest bone in the body, extending from the hip to the knee. When the femoral neck breaks, whether from repetitive stress or a sudden impact, it is a serious injury that requires prompt medical care. Without proper treatment, a fracture in this area can interrupt blood flow to the femoral head, potentially leading to complications such as avascular necrosis and long-term disability.
Start with our quick Symptom Assessment or connect directly with an Upswing Coach today.
Request an AppointmentReady to take the next step?
Start your symptom assessment or connect with a coach instantly.
Find Relief TodayOverview
The femur extends from the hip joint to the knee joint and plays a major role in standing, walking, and athletic movements. The top of the femur includes the femoral head, which fits into the pelvis to form the hip joint. Just below this is the femoral neck, a thinner section that absorbs large amounts of force with every step. Because of this stress, the femoral neck is vulnerable to injuries such as a fractured femur from trauma or a femoral neck stress fracture from overuse.
Femoral neck fractures are classified using the Garden system:
- Garden I: Partial fracture, not fully broken.
- Garden II: Complete fracture without bone displacement (nondisplaced).
- Garden III: Complete fracture with partial displacement.
- Garden IV: Complete fracture with severe displacement and bone misalignment.
Stress fractures usually begin as Garden I or II injuries but can progress to Garden III or IV if not treated early.
What causes Femoral Neck Fracture?
A femoral neck fracture can occur from two primary causes: overuse and trauma. Stress-related fractures develop from repetitive loading of the bone over time, such as long-distance running or high-impact training without adequate rest. These fractures begin as tiny cracks that worsen with continued strain. Traumatic fractures happen suddenly from intense force, such as collisions, falls, or direct blows in contact sports. Both types of injuries can result in a fractured femur, and both require immediate medical evaluation.
How the Injury Occurs
A traumatic femur fracture in the neck region usually occurs when the hip absorbs a sudden, powerful impact. This can happen during a fall, a direct collision with another player, or an unexpected twist during play. With stress fractures, the injury progresses gradually. Repetitive force on the hip, especially in activities that involve long distances, frequent jumping, or rapid acceleration, creates small cracks that eventually form a complete femoral neck stress fracture if not addressed early.
Common Everyday Causes
Although athletes are highly susceptible, non-sporting activities can also lead to a femoral neck fracture. Slipping on stairs, landing awkwardly after a misstep, or experiencing a sudden jolt can place excessive pressure on the femoral neck. Poor bone strength, low vitamin D levels, and inadequate rest between workouts can also increase the risk of a femoral neck fracture in active individuals.
Sports With the Highest Risk of Femoral Neck Stress Fractures
Stress-Related Femoral Neck Fractures
- Long-distance running: Repetitive impact and high mileage put continuous strain on the femoral neck.
- Soccer: Constant sprinting and direction changes increase repetitive stress.
- Football training: Intense preseason conditioning often overloads the femur.
- Lacrosse: Quick pivots and long runs place consistent pressure on the hip.
Traumatic Femoral Neck Fractures
- Soccer: Player collisions or falls may cause sudden hip impact.
- Hockey: High-speed contact and falls are common injury sources.
- Rugby: Tackles place strong forces on the hip and thigh.
- Football: Hard hits and awkward landings can cause acute fractures.
Symptoms
A traumatic femur fracture in the femoral neck causes immediate, sharp groin pain and an inability to bear weight. In contrast, a femoral neck stress fracture develops gradually, with symptoms that increase over days or weeks.
Common signs include:
- Groin pain that worsens with movement
- Pain in the front of the thigh
- Pain when rotating or turning the hip
- Difficulty or inability to bear weight on the injured leg
These symptoms should never be ignored, as untreated fractures can worsen quickly and lead to serious complications.
When to see a doctor
Seek urgent medical care if you experience sudden hip pain after a fall, collision, or sports injury, especially if you cannot bear weight on the leg. Do not attempt to walk or “push through” the pain.
If you notice gradual groin pain that worsens with running, standing, or walking, schedule an appointment immediately. Early detection of a femoral neck stress fracture helps prevent a full displacement or avascular necrosis.
Your doctor will examine your hip, assess your range of motion, and order X-rays. If a fracture is suspected but not visible on X-ray, an MRI can detect early stress fractures and incomplete injuries. Imaging is also used to determine the Garden classification and guide the treatment plan.
Non-operative treatment
Some femoral neck stress fractures can be treated without surgery, especially if the bone is not displaced. Non-operative care focuses on reducing stress on the injured hip and allowing the bone to heal. Treatment may include:
- Crutches: To avoid putting weight on the injured side.
- Pain-relief medication: To ease discomfort during recovery.
- Blood thinners: Often recommended after traumatic femur injuries to prevent clots.
- Physical therapy: To restore strength, mobility, and hip stability once healing begins.
This approach is reserved for early-stage, nondisplaced fractures that are closely monitored by a physician.
Try these exercises to help address your condition:
Below is a PDF of the Exercise Program
Surgical Treatment
Most displaced femoral neck fractures and some nondisplaced fractures require surgery. Treatment options depend on bone alignment, the severity of the fracture, and the patient’s age and activity level.
Common surgical options(open reduction include:
- Open Reduction and Internal Fixation(ORIF)
The surgeon realigns the bone without making a large incision, then uses cannulated screws to stabilize the fractured femur For more severe fractures, this open procedure repositions broken bone fragments and secures them with screws or plates.
- Partial Hip Replacement (Hemiarthroplasty)
A prosthetic device replaces the femoral head and neck when the fracture is severely displaced or the bone cannot be repaired.
- Total Hip Replacement (THR)
Both the femoral head/neck and the hip socket are replaced. This is often required for Garden IV fractures or when avascular necrosis develops.
Recovery
Recovery depends on the severity of the fracture and the type of treatment. After open reduction and internal fixation surgery, patients usually use crutches or a walker for several weeks and may require assistance with daily tasks. Those who undergo partial or total hip replacement may begin weight-bearing sooner.
Return to normal activities may take 2 to 6 months, depending on healing progress. Physical therapy is essential to restore hip flexibility, strength, and endurance. Athletes recovering from a femoral neck stress fracture can often return to sports with modifications, while those with major traumatic fractures must follow their surgeon’s guidance closely before resuming high-impact activities.
Dr. Jay Kimmel is a board-certified orthopedic surgeon specializing in sports medicine, arthroscopic surgery, and shoulder and knee disorders. He completed his orthopedic training at New York-Presbyterian/Columbia University Medical Center and a Sports Medicine Fellowship at Temple University.
Dr. Kimmel previously served as the Director of the Connecticut Sports Medicine Institute at Saint Francis Hospital and has held faculty appointments as Clinical Assistant Professor in the Departments of Orthopedics and Family Medicine at the University of Connecticut. He has extensive experience caring for athletes as a team physician for high school and collegiate programs and continues to teach in the athletic training departments at Westfield State University and Springfield College.
Find the Support You Need — Right When You Need It
Whether you’re managing pain for the first time, need ongoing guidance, or require expert medical care, we’re here to help you every step of the way.
ORTHO DIRECT
Video visit with an orthopedic doctor for advice and a care plan.
$30
/MonthMRI DIRECT
Fast, affordable MRI with orthopedic review. No insurance required.
$499
/MonthFrequently Asked Questions
How do I know if I have a neck of femur fracture?
Groin pain, thigh pain, and difficulty bearing weight are common warning signs. Imaging tests such as X-rays or MRI confirm the diagnosis.
Is a femoral neck fracture life-threatening or disabling?
If left untreated, it can lead to avascular necrosis and long-term hip problems. Early treatment significantly reduces the risk of complications.
How long does recovery take after a femur fracture?
Most patients recover within 1–4 months, depending on the severity and treatment approach. Physical therapy plays an important role in recovery.
Can athletes return to sports after a femoral neck fracture?
Yes. With proper healing and rehabilitation, many athletes safely return to their sport. Your surgeon and physical therapist will guide the timing.